This is an article that Dr Roshini wrote for ‘acute matters which was a HSN newsletter that goes out to GP’s’ which talks about CKD(chronic kidney disease). Read part of the article and download it in full as PDF file.
Worldwide, CKD is a recognised health burden with increasing number of patients commencing renal replacement therapy (RRT). CKD leads to significant morbidity and mortality with a large contribution from cardiovascular complications. Early detection of CKD is the key in preventing progression of renal impairment and attendant comorbidities.
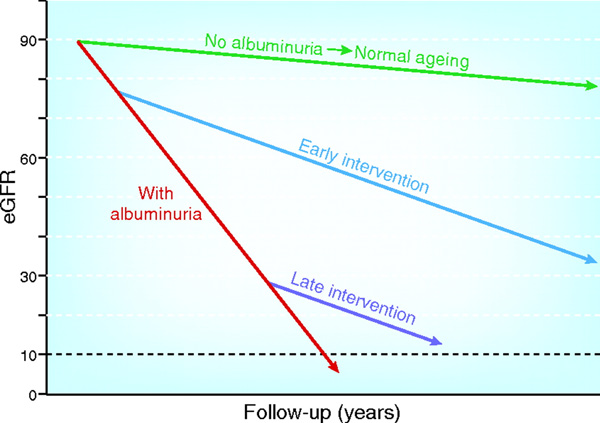
CKD is defined as abnormalities of kidney structure or function reflected by a glomerular filtration rate (GFR) of <60ml/min/1.73 m2 for 3 months 1. Microalbuminuria has been incorporated into the staging of CKD to stratify individuals at added risk of progression to End Stage Renal Failure (ESRF) ie a GFR <15 ml/min/1.73m2. Early intervention to reduce albuminuria prevents a rapid decline in eGFR shown in Figure 12.